


Neighbor Tuesday: Global child deaths at historic low

Children’s global health is what I do in my day-job at Duke. And, I love it! I know I’ve said it before, but I still pinch myself that I’m doing this work at all. This job and the collabo-friends are a dream!
The United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) just released its 2023 report. I was holding my breath for this one because COVID wrecked many of our global health advances made in the past few decades, particularly for children. Although high-income countries have recovered fairly well, low-income countries have not. And, usually that means that the most vulnerable are affected the most in these countries - namely, children and women.
Let me give you a little background on the UN IGME first. This is an inter-agency group formed in 2004 to improve child mortality and led by the UN Children’s Fund (UNICEF), the WHO, the World Bank Group, and the UN Population Division of the Department of Economic and Social Affairs. I particularly love the UN IGME because they focus on how data can be used for good - so, neighboring data.
Now back to the report. They estimated that children deaths (children under 5) dropped to 4.9 million in 2022.

That’s still a lot of children dying. But, historically, we are making strides. Look at the deaths from 1990-2022 in the chart below. You can definitely tell the decline has been steady.

However, it depends on where you live. For children in sub-Saharan Africa, the risk of dying is 18 times HIGHER than Australia or New Zealand. If you compare children in countries with the highest-mortality rates the risk is a STAGGERING 80 times than children in the lowest-mortality countries.

What’s going on and what can we do?
When you tease the data apart, you see some clues on what’s going on.
Under-five mortality is still concentrated in the neonatal period (the first 28 days of life). Of the total under-five deaths, 41% occurred during the first 28 days of life in 2000. Now, we would hope that percentage would be reduced 20 years later in this report, right? But, we see the opposite. Now, we are at 47%. Birth and the neonatal period continue to be a high-risk time, especially if you do not have good healthcare access. For example, my work deals with surgical conditions for the child. If you read my book, you heard me talk about a condition called gastroschisis. It’s a horrific condition where the bowels are born outside of the body where the belly button is. In the US or other high-income areas, you can see this condition on an ultrasound scan prior to birth. So, you can prepare with a pediatric surgeon ready to go when the baby is delivered. The baby has a >95% chance of survival with no complications. In low-income countries, though, the chance of dying is the same percentage - 95-100%. And, that death occurs within a few days of birth. Getting that child to a well-equipped hospital with a pediatric surgeon available in a timely manner is critical. That often is not the case in places where I work. In the book, I talked about Ghana and Somaliland and Burundi and defined it as structural violence. That chapter continues to really resonate with people. So, more needs to be done for the smallest babies and their moms. We are going backwards.
The declines in under-5 mortality depends on where you live. In the graph below, look to the far-right at the World’s under-five mortality rates. You can see the decline from 1990 to 2022. Look at the 2022 number - 37%. Now go look to the far-left at Sub-Saharan Africa. They have made fantastic declines! BUT, the 2022 rate is still 71% - double the world’s rate. As an epidemiologist, this is the data we look for. The news article about the report says, “Sub-Saharan Africa has reduced the under-five mortality rates dramatically over the past 30 years.” That’s right! But, we need to compare that to other regions or the rest of the world to see the true comparison. There’s still quite a bit of work to do.

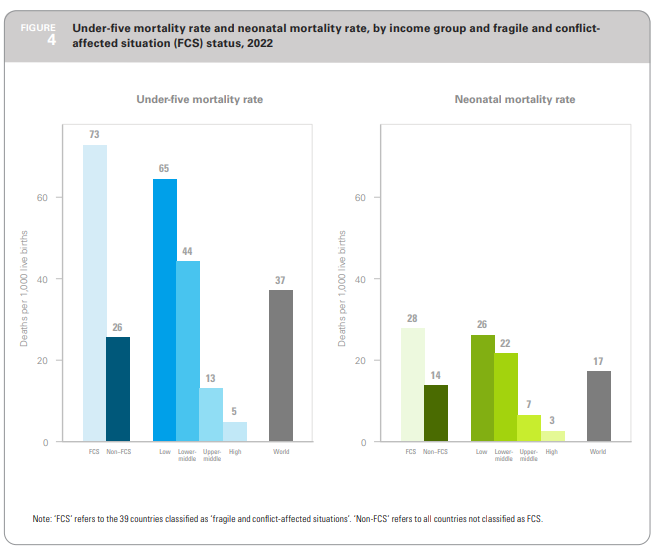
Children in conflict areas and fragile countries are especially vulnerable. The World Bank classifies countries with high levels of social fragility and violent conflict (FCS). The report found that the under-five mortality rates in FCS areas was TRIPLE the rate of non-FCS countries. 50% of the world’s under-five deaths occurred in FCS countries. We know this anecdotally, don’t we? We see it on the news or read about it. But the power of data brings that anecdote to paper in a way that hopefully gets people’s attention. My team and I are working on a project aimed at improving children’s cancer care in conflict zones. I cannot wait to share more of that with you as the analysis is finished. We are also hoping that we can make a strong case for protecting health systems in conflict zones, especially for children. The devastation to health systems in places like Gaza and the Sudan are maddening, mind-boggling, and certainly not neighborly.

Most deaths in low-income areas are still from preventable causes. This one gets me every time. If you live in the US like I do, we rarely see deaths from malaria, diarrhea, measles. But in Sub-Saharan Africa or Southern Asia, those are still in the top 10 the leading cases. The chart below shows the percentage decline in deaths for these conditions, worldwide and in Sub-Saharan Africa or Southern Asia. Again, we want to celebrate those declines. I have many friends, as I’m sure you might too, that are working tirelessly in these countries to treat malaria, pneumonia, or measles in low-income countries. And, Also. We still have some work to do.

This leads me to…


Then, what do we do about it?
If the current trends keep going, 59 countries will not meet the Sustainable Development Goals for under-five mortality.

The goal is at least as low as 25 deaths per 1,000 low births. Right now, the US is 6.2. Somalia is 117. Venezuala is 24. Of the 59 countries, 43 need to double their current rate of progress. To meet the SDG in 2030, the report advocated for 7 actions steps. You can read all of them, but I want to highlight a few:

Invest in local communities. If you look at the literature at what works to protect children, interventions designed, planned, and implemented by the local communities work the best. The report gives an example of training skilled birth attendants and local midwives in care around the time of birth and during the critical first 28 days of life. If community-based child survival interventions were scaled up to reach 90% of children in their countries, deaths could drop by 30%! That would definitely help accelerate the SDG goals in countries with the greatest needs.
Invest in health systems. Babies in need most often require swift care. Like in the example of gastroschisis above, that baby needs to get to care quickly. A strong health system means that community-health workers can quickly link the mom to a district hospital which can then refer to a tertiary level hospital to perform the surgery. Investments in health systems as a whole has a massive return of investment to the country too. At least a 10:1 return of investment! That’s what a lot of my studies look at and the data is clear - healthy children means thriving societies.
Protect families from health expenditures. My work deals with families having to make a choice between healthcare for one child and food for the rest. Universal health coverage would make that question obsolete. If you’ve read my book, you read about me going to the United Nations to advocate for the inclusion of surgical care into existing universal health coverage plans. My data clearly shows in multiple studies that families are bankrupted if they have a child with a health need. What if we can do something about that for the world’s children? To me, that’s why universal health coverage matters.
Neighboring to the most vulnerable children in the world requires solidarity, compassion, and recognition. It also requires data. The report ends with advocating for better data on child mortality so we can then meet the real needs. To me, that sounds a lot like the Good Samaritan story and not walking by. That’s what epidemiology is to me - quantifying who is at need on the side of the road and then choosing to not walk by - hence, I titled my book on epidemiology and global health, The Science of the Good Samaritan.
If you’re reading this, I have a hunch that you’re already there with solidarity and compassion. Next time, we’ll talk about how to match today’s posts with voting like a neighboring in light of this data.
Until then, take good care of yourselves. I’m grateful to have you all as neighbors!
-Emily
PS: For more reading, you might enjoy this NPR Goats and Soda article on Dr. Joel Breman. He was an Ebola pioneer and a champion of doing global health well, including efforts towards smallpox control. I thought the article was a beautiful recognition of a life well lived.