


Neighbor Tuesdays: Global childhood cancer

Hello from Neighbor Tuesday: Global edition. =) Many of you know that I work in Somaliland, Burundi, and Tanzania and that I traveled to Tanzania earlier this year a few times - 1 trip with my hubs and the other with the hubs and kids…and COVID. ugh. (Click on the links to read about those incredible trips to catch up.)
What am I doing in Tanzania? I’d love to tell you…
I am working with the local providers who treat children with cancer in Tanzania. We know that the inequity difference of children surviving from cancer between high-income countries (like the US) and lower-income countries (like Tanzania) is one of the starkest in global health.
The percentage of children dying from cancer in lower-income countries is the same as children surviving in high-income countries. We call this the 80-20 gap.

What I want you to do before we go on is think with me why this is the case and if there’s anything we can do about it. Sometimes when we hear these statistics, it’s easy to move on because the problem is either too big or it feels like we in our normal lives can’t do anything about it. For childhood cancer, it’s pretty clear what we need to do though.
If we look back at the US in the 1950s, the majority of cancers had an 80% mortality rate. Sounds like the current mortality rate for lower-income countries, doesn’t it?

Since the 1950s, we have made dramatic improvements for all childhood cancer types. Resulting in the 80-20 gap worldwide. So, what changed? Or in other words, can lower-income countries do the same?
“The field of pediatric oncology has seen more progress than almost any other clinical area in the last Fifty years.” (Link to full article here)

Clap clap clap and more claps to the researchers and oncologists and advocates who paved the way for that last sentence. I wanted to quote it because it shows that improvements in childhood cancer survival can be made and have been made - “more than almost any other clinical area in the last 50 years”. Those improvements include advances in treatments, improvements in early diagnosis and the start of treatment, and supportive care when the littles are feeling crummy from the treatment. And, they have worked!
So, why haven’t these improvements been made in the places that need it the most? If we look globally, there are over 400,000 cases of childhood cancer per year - and over 90% of them are in lower income countries. That statement gets me every time I write it. 90% is where the burden is, but not the investment. Billions of dollars have been spent on childhood cancer research, treatments, and prevention, but only 5% have gone to support healthcare delivery (like making sure children can get to the care they need when they need it). Additionally, 78% of the billions are allocated to institutions based in the US. Now, I just mentioned that dramatic improvements have been made in childhood cancer in the US - so those billions are definitely worth it. But, between 2008 and 2016, no grant was given to institutions in Southeast Asia and only one in Africa (Egypt) based on a systematic review in the Lancet. There’s a mismatch then between countries with the highest burden and funding to alleviate that burden.
We have improved the survival of children with cancer in the US and other high-income countries. Now it’s time to do that in other countries. That’s equity. We know the roadmap.
So, what can we do?
Fund where the need is most - I head to the United Nations General Assembly in September and there always lots of policy makers, country leaders, and money people. Billions of dollars are allocated to overcome huge global problems, and I hope they allocate more towards strengthening health systems for children with cancer in countries that need it most. To be fair, there are lots of global problems - climate change, hunger, pandemic preparedness, women’s health. The thing about health system strengthening is that it affects most of those issues. You improve health systems and referral networks in the country, you improve children’s health, including cancer, women’s health like prenatal care, pandemic response with strong testing and diagnostic capabilities, etc. Strengthening the health system does mean increasing doctors and nurses, for sure. And, also. It means making sure treatments are available, cold chains for vaccines are possible, oxygen and anesthesia are on-hand, electricity is reliable…That’s what the US did over the past 50 years for children. I’d love to see it also done for the rest of the world’s children. So, speaking of health systems…
Bolster health systems - Think with me through a scenario with a family. One of the children starts developing symptoms they are sick and the parent notices. They want to take the child to a doctor for a timely diagnosis and start of treatment. In order to get a timely diagnosis, you need the tests, the laboratories, the physicians, the radiologists, etc. Unfortunately, those health system factors are not nearly as readily available in lower-income countries.
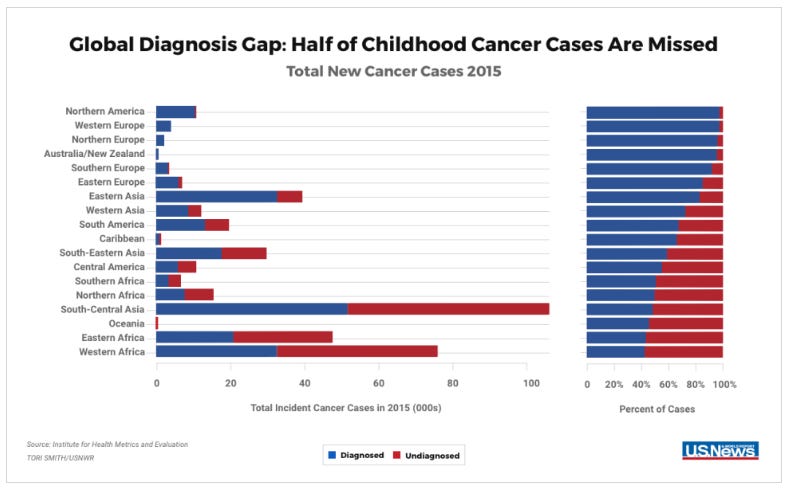
Check out the figure below. On the left are new cases of childhood cancer in different countries and on the right are cases are missed. This is also only a part of the cancer care story for these families. Even if the children are diagnosed timely, the treatment and follow-up care needs to be available - and available in a way that doesn’t bankrupt the family with high healthcare costs. Next month, I join others at the United Nations General Assembly meetings on universal health advocacy - to ensure families don’t have to choose between providing health care to one child or feeding the rest of the family. Being a good neighbor to me means making sure no family has to ask that question.

Think and act like a global neighbor - This doesn’t mean that we (if you live in a high-income country) zoom in with White Saviorism to “fix” a problem. This means we work alongside the in-country providers in a truly equitable partnership. Dr. Paul Farmer calls this ‘accompaniment’ - It’s walking alongside people as equals and respecting cultures and traditions. It’s not ‘othering’ another group, but rather honoring them. I call it a “withness” in my upcoming book. It’s a way of centering our minds and hearts towards our neighbors that pulls down walls of unconscious bias that so easily seeps into America.
For childhood cancer, we have a roadmap of what works to dramatically improve survival. Now, we need the solidarity, empathy, and political will to think and act like a global neighbor. That includes who we vote for (more on that in a later Neighbor Tuesday post since we are entering an election year in the US).
For me, I’m looking forward to working with my team to do a small part of that in Tanzania.
-Emily
For whatever reason I’m just seeing this, so my comment is way late.
Cancer and specifically childhood cancer is my area of research and passion.
I think if we treated cancer the way we treated AIDS that would go a long way. With the help of President Bush poor African countries have been able to get the medicine needed to fight HIV/AIDS and a huge dent has been made there, so if we treated cancer like that I believe we could make enormous headway in helping these less wealthy countries fight and the survival rates would skyrocket.
I agree with all of your points. I think the biggest one is treating other countries around the world both wealthy and not as wealthy as neighbors, that one is so important and I hope we can start doing that.
I like "withness." It's a great word to sum up what it means to care for people in so many ways.